Hi. I'm Blaise ₍⸍⸌̣ʷ̣̫⸍̣⸌₎ I like cats more than I like people. Stigma Fighter & Mental Health Advocate Destigmatizing Borderline Personality Disorder.
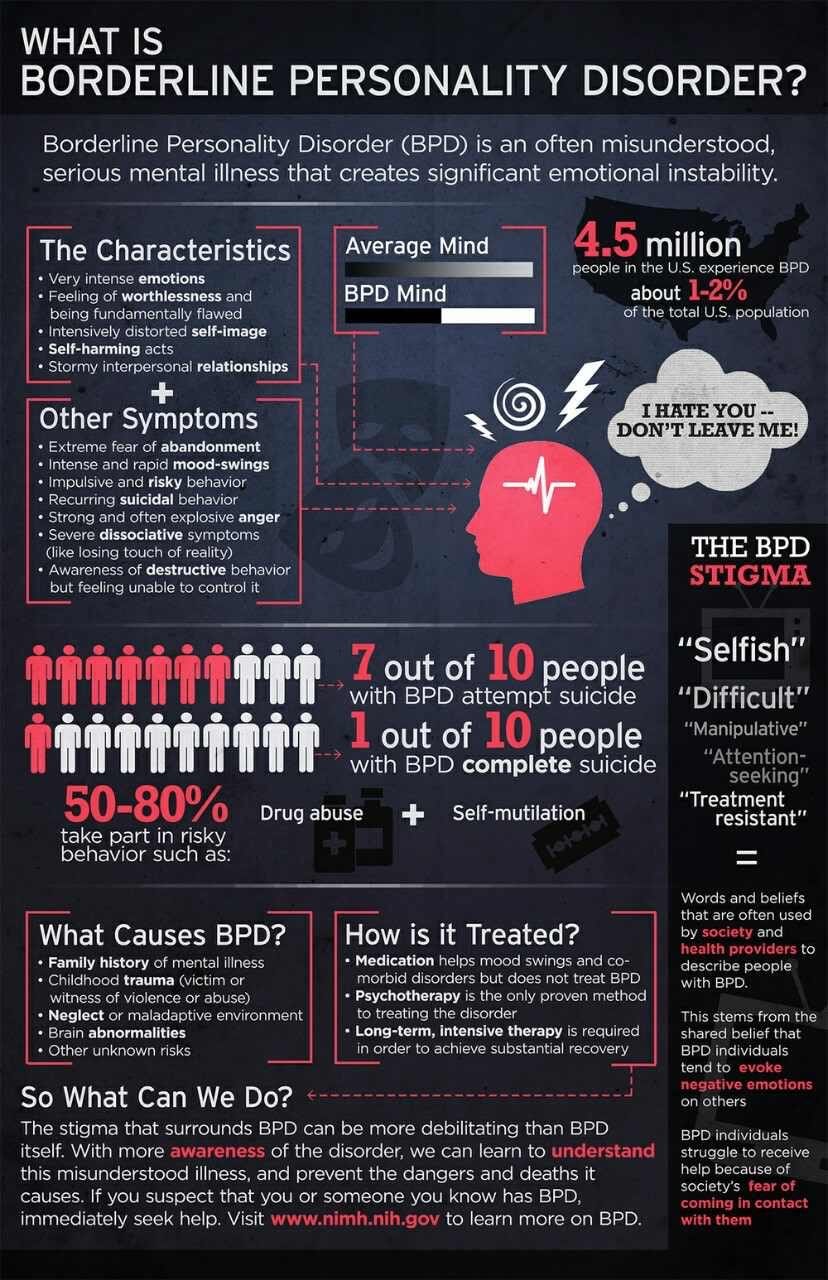
Borderline Personality Disorder is one of the most misunderstood, stigmatised & complex mental health diagnoses.
One could write pages relating to the condition BPD and a layman’s understanding would still be incomplete.
For this reason I am going to try and keep it short, simple and concise as I can and explain to you what BPD is to me.
BPD is intense feelings of loneliness & an inability to sit with myself without resorting to poor coping behaviours.
BPD is extreme emotional vulnerability & sensitivity. Feelings of severe internal distress are triggered easily.
BPD causes a slow return to my baseline. This means strong emotions & cognitions tend to take a long time to dissipate.
BPD feels like I am ‘dying inside’ immense emotional turbulence & pain, distress beyond explanation.
BPD is feeling as though my emotions are so impossible to live with that they will surely kill me. Most of the time it feels as though my emotions are in control of me and I am not in control of my emotional world.
BPD is impulsive behaviours and an inability to ‘think before I act’ and ‘learn from my mistakes’ time and time again.
BPD is extreme & rapid mood swings ranging from periods of depression to somewhat dysphoric & delusional bouts of mania.
BPD is paranoia and anxiety, especially in interpersonal circumstances.
Problems with ‘attachment’ especially with authority & care-giver figures e.g. therapists, teachers, etc.
A history of suicidal ideation, tendencies & threats. Multiple short & long-term admissions to A&E, hospital and crisis houses.
Risk-taking & thrill-seeking behaviours as well as chronic boundary-pushing & rule-breaking, especially with authority.
Self-destructive tendencies, especially self-injurious behaviour mostly through cutting. This has also manifested through eating disordered behaviours, alcohol & drug abuse. Others may struggle with sex, spending, gambling & other addictive behaviours.
Lack of sense of self. Having to define myself based on my external world & lacking a fundamental secure sense of a ‘true me’, only being able to have an idea of who I am by looking at evidence & cues in the people & world around me. Only being able to have an idea of who I am by looking at evidence & cues in the people & world around me.
BPD is depersonalisation (feeling as though I do not exist, am not in my body & am not in control of thoughts/actions).
Difficulties with appropriately expressing my anger often leading to heightened displays & outbursts of intense pent-up emotion.
A highly severe guilt & shame complex in response to every imperfect interaction or perceived personal failure.
Feelings of self-hatred, self-loathing, hopelessness, despair, especially in response to making mistakes that impact others.
Black-and-white thinking as well as the tendency to engage in catastrophic thinking, mind-reading & jumping to conclusions.
High perceptiveness of people and circumstances around me, to the point of unhealthy & paranoid hyper-vigilance.
Feelings of being misunderstood by the world & people around me & of never fitting in, always being on a different wave-length.
Splitting: Rapidly changing perceptions of myself & people around me from one extreme to the other.
Finally manipulative behaviours such as playing people in my life off against each other. Asking multiple people the same thing until I receive the answer I am looking for, convolutedly threatening self-destructive.
I wouldn’t be like this if I knew how to not be like this. When you’re fighting BPD, you’re fighting a silent battle. No one sees how hard you’re constantly having to fight your mind.
People with the diagnosis of BPD need to be heard. We are all too often silenced by services & professionals.
People with BPD are not a bunch of stereotypes. We have emotions, feelings, dreams like everyone else. We just feel too deeply.
Living with BPD or people who have it is a blessing and learning curve in itself. Stay patient, focus and appreciative.
People with BPD are many things. Often loving, kind, passionate, creative, determined, giving, ambitious, brave and caring.
The stigma around BPD is so wrong. 99% of the people I’ve come in to contact with are absolutely loving, giving and caring.
For more information and support, follow my Twitter BPDBanter
Hi. I'm Blaise ₍⸍⸌̣ʷ̣̫⸍̣⸌₎ I like cats more than I like people. Stigma Fighter & Mental Health Advocate Destigmatizing Borderline Personality Disorder.
The concept of schizophrenia is dying. Harried for decades by psychology, it now appears to have been fatally wounded by psychiatry, the very profession that once sustained it. Its passing will not be mourned.
Part of the problem turns out to be the concept of schizophrenia itself.
Arguments that schizophrenia is a distinct disease have been “fatally undermined.” Just as we now have the concept of autism spectrum disorder, psychosis (typically characterized by distressing hallucinations, delusions, and confused thoughts) is also argued to exist along a continuum and in degrees. Schizophrenia is the severe end of a spectrum or continuum of experiences.
Jim van Os, a professor of psychiatry at Maastricht University, has argued that we cannot shift to this new way of thinking without changing our language. As such, he proposes the term schizophrenia “should be abolished.” In its place, he suggests the concept of a psychosis spectrum disorder.
Another problem is that schizophrenia is portrayed as a “hopeless chronic brain disease.” As a result, some people given this diagnosis, and some parents, have been told cancer would have been preferable, as it would be easier to cure. Yet this view of schizophrenia is only possible by excluding people who do have positive outcomes. For example, some who recover are effectively told that “it mustn’t have been schizophrenia after all.”
Schizophrenia, when understood as a discrete, hopeless and deteriorating brain disease, argues van Os, “does not exist.”
I expect to see the end of the concept of schizophrenia soon...the syndrome is already beginning to breakdown, for example, into those cases caused by copy number [genetic] variations, drug abuse, social adversity, etc. Presumably this process will accelerate, and the term “schizophrenia” will be confined to history, like “dropsy.”
Research is now exploring the different ways people may end up with many of the experiences deemed characteristic of schizophrenia: hallucinations, delusions, disorganized thinking and behavior, apathy and flat emotion.
Indeed, one past error has been to mistake a path for the path or, more commonly, to mistake a back road for a motorway. For example, based on their work on the parasite Toxoplasma gondii, which is transmitted to humans via cats, researchers E. Fuller Torrey and Robert Yolken have argued that “the most important etiological agent [cause of schizophrenia] may turn out to be a contagious cat.” It will not.
Evidence does suggest that exposure to Toxoplasma gondii when young can increase the odds of someone being diagnosed with schizophrenia. However, the size of this effect involves less than a twofold increase in the odds of someone being diagnosed with schizophrenia. This is, at best, comparable to other risk factors, and probably much lower.
Compared with noncannabis users, the daily use of high-potency, skunk-like cannabis is associated with a fivefold increase in the odds of someone developing psychosis. Compared with someone who has not suffered trauma, those who have suffered five different types of trauma (including sexual and physical abuse) see their odds of developing psychosis increase more than 50-fold.
Other routes to “schizophrenia” are also being identified. Around 1 percent of cases appear to stem from the deletion of a small stretch of DNA on chromosome 22, referred to as 22q11.2 deletion syndrome. It is also possible that a low single digit percentage of people with a schizophrenia diagnosis may have their experiences grounded in inflammation of the brain caused by autoimmune disorders, such as anti-NMDA receptor encephalitis, although this remains controversial.
All the factors above could lead to similar experiences, which we in our infancy have put into a bucket called schizophrenia. One person’s experiences may result from a brain disorder with a strong genetic basis, potentially driven by an exaggeration of the normal process of pruning connections between brain cells that happens during adolescence. Another person’s experiences may be due to a complex post-traumatic reaction. Such internal and external factors could also work in combination.
Either way, it turns out that the two extreme camps in the schizophrenia wars—those who view it as a genetically-based neurodevelopmental disorder and those who view it as a response to psychosocial factors, such as adversity—both had parts of the puzzle. The idea that schizophrenia was a single thing, reached by a single route, contributed to this conflict.
Implications for treatment
Many medical conditions, such as diabetes and hypertension, can be reached by multiple routes that nevertheless impact the same biological pathways and respond to the same treatment. Schizophrenia could be like this. Indeed, it has been argued that the many different causes of schizophrenia discussed above may all have a common final effect: increased levels of dopamine.
If so, the debate about breaking schizophrenia down by factors that lead to it would be somewhat academic, as it would not guide treatment. However, there is emerging evidence that different routes to experiences currently deemed indicative of schizophrenia may need different treatments.
Preliminary evidence suggests that people with a history of childhood trauma who are diagnosed with schizophrenia are less likely to be helped by antipsychotic drugs. However, more research into this is needed and, of course, anyone taking antipsychotics should not stop taking them without medical advice. It has also been suggested that if some cases of schizophrenia are actually a form of autoimmune encephalitis, then the most effective treatment could be immunotherapy (such as corticosteroids) and plasma exchange (washing of the blood).
Yet the emerging picture here is unclear. Some new interventions, such as the family-therapy based Open Dialogue approach, show promise for a wide range of people with schizophrenia diagnoses. Both general interventions and specific ones, tailored to someone’s personal route to the experiences associated with schizophrenia, may be needed. This makes it critical to test for and ask people about all potentially relevant causes. This includes childhood abuse, which is still not being routinely asked about and identified.
The potential for different treatments to work for different people further explains the schizophrenia wars. The psychiatrist, patient or family who see dramatic beneficial effects of antipsychotic drugs naturally evangelically advocate for this approach. The psychiatrist, patient or family who see drugs not working, but alternative approaches appearing to help, laud these. Each group sees the other as denying an approach that they have experienced to work. Such passionate advocacy is to be applauded, up to the point at which people are denied another approach that may work for them.
What comes next?
None of this is to say the concept of schizophrenia has no use. Many psychiatrists still see it as a useful clinical syndrome that helps define a group of people with clear health needs. Here it is viewed as defining a biology that is not yet understood but which shares a common and substantial genetic basis across many patients.
Some people who receive a diagnosis of schizophrenia will find it helpful. It can help them access treatment. It can enhance support from family and friends. It can give a name to the problems they have. It can indicate they are experiencing an illness and not a personal failing. Of course, many do not find this diagnosis helpful. We need to retain the benefits and discard the negatives of the term schizophrenia, as we move into a post-schizophrenia era.
What this will look like is unclear. Japan recently renamed schizophrenia as “integration disorder.” We have seen the idea of a new “psychosis spectrum disorder.” However, historically, the classification of diseases in psychiatry has been argued to be the outcome of a struggle in which “the most famous and articulate professor won.” The future must be based on evidence and a conversation that include the perspectives of people who suffer—and cope well with—these experiences.
Whatever emerges from the ashes of schizophrenia, it must provide better ways to help those struggling with very real experiences.
Editor’s Note: Every whiff you take not only brings a cloud of chemicals swirling up your nose, but matters to your experience of taste as well as smell. Scientists studying smell have not only provided compelling evidence that it’s more sophisticated than previously thought, but believe that the sense of smell impacts our mood and behavior and has the potential to detect and treat some neurological disorders. Compared to other senses, smell has long been underappreciated, writes our author, but that is now beginning to change.
Illustration by William Hogan
In many ways, the sense of smell—also known as olfaction (from the Latin word for smell or odor, olfactorius)—is our most complex sensory system, capable of distinguishing thousands, if not millions, of different odors, often at concentrations below those detectable by sophisticated instruments. The biological machinery required for such a feat is remarkable, involving six to ten million odorant receptor cells embedded within a thin layer of tissue (epithelium) high in the nasal chambers. Each receptor cell projects 10 to 30 thread-like cilia into the mucus covering the epithelium (see figure 1 below).
These cilia carry receptors—protein structures specialized to respond to odor-carrying molecules, termed odorants. There are nearly 400 types of receptors, different subsets of which are triggered by different odorants. Each of the olfactory receptor cells contains only one type of receptor. When enough odorant molecules get through the mucus layer and bind to the receptors located on the receptor cell cilia, they stimulate a neural impulse. The pattern of activated receptors is specific to a given odorant, and the neural impulses that are generated are decoded by higher brain regions. Memory processes also become involved, allowing us to recognize odor sensations of which we are familiar.
The major breakthrough for understanding the first phase of olfactory transduction came in 1991 when Linda Buck and Richard Axel at Columbia University published their seminal paper identifying the gene family responsible for the expression of the olfactory receptors.1 Their work, which led to the 2004 Nobel Prize in Medicine or Physiology, put to rest questions as to the nature of initial olfactory transduction that had puzzled scientists for hundreds of years.
Since then the situation has become much more complex, with ever more types of receptors being found on some olfactory receptor cells,2 and the realization that olfactory receptors are present in tissues throughout the body. These include the skin,3 skeletal muscle,4 thyroid,5 heart,6 lungs,7 pancreas,8 thymus,9 prostate,10 kidney,11 bladder,9 testes,5 intestine,12 blood vessels,13 and ganglia of the autonomic nervous system.13 Their widespread distribution raises the question of whether these receptors should, indeed, be called “olfactory.“ Depending upon their location, they are involved in many biological and physiological processes, including glucose homeostasis, lung ventilation, regulation of blood pressure, mitigation of tumor progression, promotion of angiogenesis, facilitation of sperm motility, induction of wound healing, and alteration of gut motility and secretion.14 Understanding the role of such receptors in these diverse processes is opening new vistas for novel pharmacological approaches to disease management and treatment.
The Underrated Sense
Although most of us take our sense of smell for granted, it is critical for our well-being. We use olfaction to verify the cleanliness of our clothes and homes, and to fully enjoy foods, beverages, personal care products, flowers, and other aspects of our environment. Without a sense of smell, we are exposed to the dangers of spoiled food, leaking natural gas, burning electrical wires, smoke, and other environmental hazards. The sense of smell is so important that those who can’t smell (anosmics) are disqualified for “appointment, enlistment, and induction” into the US Armed Forces. Indeed, the lack of smell ability can be the basis for retirement or discharge.15
Multiple factors influence our ability to smell. These include occupation (e.g., perfumers and master sommeliers perform better than most of us on olfactory tests), sex, age, exercise, smoking, nutrition, head trauma, disease, and exposures to viruses, bacteria, and xenobiotics.16 The influence of age on smell function is particularly salient. More than three-quarters of individuals over the age of 80 have a demonstrable smell problem, usually reduced sensitivity.17 This decrease is illustrated below (see Figure 2 below), where a major drop occurs in later life in scores on the University of Pennsylvania Smell Identification Test (UPSIT), a 40-odor smell test developed at our center in the early 1980s (Figure 3).18 (Note in Figure 2 that women, on average, outperform men on this test and maintain their superiority into later life.) Over the age of 85 years, 40 percent of men and 26 percent of women are anosmic, i.e., have no sense of smell at all.19
Figure 2. University of Pennsylvania Smell Identification (UPSIT) scores as a function of age and sex. Note that women identify odorants better than men at all ages although significant overlap occurs. Numbers by data points indicate sample sizes. (From Doty and colleagues.17 Copyright 1984 American Association for the Advancement of Science.)
It is noteworthy that many patients who come to our center’s clinic for evaluation and treatment do not recognize that they have a smell problem, complaining only of a “taste” problem. However, when we formally test them, their ability to smell proves to be the culprit. Why? Because the taste buds, located throughout the oral cavity but primarily on the tongue, sense only sweet, sour, bitter, salty, and savory (“umami) sensations. Everything else we think of as taste, such as strawberry, apple, chocolate, coffee, butterscotch, meat sauce, and apple pie, are really flavors that depend upon the sense of smell.
This is easily demonstrated. The next time you sip your coffee, pinch your nose closed while swishing the coffee around in your mouth. You will notice the bitterness of the coffee, its warmth and smoothness, but not the distinctive coffee flavor. Indeed, the sensation is much like swishing bitter hot water. The reason why the coffee “taste” disappears is that, by holding your nose shut, you block the flow of coffee flavor molecules from the rear of the oral cavity to the olfactory receptors via the nasopharyx, the opening from the mouth into the nose.
I was once asked to visit a large retirement home to better understand why there was concern about bad tasting food. The situation was quite dire, since some residents had largely refused to eat the food and a few were wasting away. Such turmoil arose around this issue that many of the residents were on a campaign to have the chef fired. The chef eventually quit, but the problem continued even after a new chef had come on board. I had the opportunity to give a lecture to 100 or so of the residents on nutrition and the chemical senses, and passed out the UPSIT for them to take immediately after my talk. It was at this time that most of the residents discovered they could not smell very well, with most exhibiting hyposmia (decreased smell function), and that the problem with the institution’s food was largely in their noses, not in the kitchen!
Smelling Danger
Aside from altered perception of the flavor of foods and attendant nutritional issues, the loss of smell function that most of us experience in our later years has potentially lethal consequences. This is evidenced by the disproportionate number of elderly people who have died in accidental gas poisonings, in part because of their inability to detect the odor added as a safety factor to natural gas.20 Most of us have, at some time in our lives, used this sense to avert a danger from something burning on the stove, a smoldering wire in an electrical outlet, or gas from a stove that was not completely turned off. In a study of over 1,000 persons conducted by the Medical College of Virginia, anosmics were three times more likely than those with a normal sense of smell to report having experienced a potentially life-threatening event such as the ingestion of spoiled food or a failure to detect smoke or leaking natural gas.21
Recent studies suggest that smell loss is an extremely strong risk factor for death in healthy older persons, increasing the odds of dying by more than 300 percent over a four-to five-year period.22 Although the reasons behind the association have yet to be determined, smell loss is a stronger predictor of death than cognitive deficits, cancer, stroke, lung disease, or hypertension, even after controlling for sex, age, race, education, socioeconomic status, smoking behavior, cardiovascular disease, diabetes, and liver damage.22, 23
Independent of age, we now know that smell dysfunction heralds the onset of a number of neurological diseases, including Alzheimer’s and Parkinson’s diseases.24 In some cases, such dysfunction occurs years, even decades, before the appearance of the classic disease symptoms. The olfactory bulb—a structure at the base of the brain that receives information from the olfactory receptor neurons—is among the two brain regions that first show disease-related pathology in Parkinson’s disease.25 Although damage to the olfactory bulb also occurs in early Alzheimer’s disease, some studies suggest that disrupted connections between the olfactory cortex and the hippocampus, which is involved in memory, predate it.25 Factors including damage to neurotransmitter systems critical for olfactory function may precede the development of the neuropathology of such diseases, possibly even catalyzing disease development itself.26
Impact on Memory
We and others have observed a close relationship between the ability to smell and memory: older persons with olfactory loss are more likely to report difficulties in memory.27 In a study of 1,092 non-demented elderly persons (average age 80 years) from a multi-ethnic community in New York, UPSIT scores varied with the degree of memory impairment and with performance on a number of cognitive tests.28 Importantly, such scores were weakly correlated with the MRI-determined volume of the hippocampus, a brain structure intimately associated with memory.
Numerous longitudinal studies have demonstrated that olfactory deficits are associated with future cognitive decline and Alzheimer’s disease in older populations.29 Moreover, interactions with genetics have also been demonstrated. In 1999, Amy Bornstein Graves and her associates at the University of South Florida published a pioneering study in which a 12-odor version of the UPSIT was administered to 1,604 community-dwelling senior citizens. None initially showed any signs of dementia.30 The smell test scores were found to be a better predictor of cognitive decline over the study’s two-year period than scores on a global cognitive test. Persons with normal smell function who carried one or two APOE-4 alleles (a risk factor for Alzheimer’s disease) had only a slight elevation in risk of developing cognitive decline. However, anosmic carriers of such alleles had a five-fold risk in developing cognitive decline during this time period. While this risk was approximately three-fold in men, it was nearly 10-fold in women.
Close relatives of patients with Alzheimer’s disease appear to have poorer smell function than non-relatives of the same sex and age, implying that genetic factors may be at play.31 However, the potential influences of interactions between environmental factors and genes, including the APOE-4 allele, cannot be overlooked. Using the UPSIT, Calderon-Garciduenas and her colleagues in Mexico City found olfactory dysfunction in 35.5 percent of 62 young persons (average age 21 years) living in a highly polluted area of that city, as compared to only 12 percent of those living in a much less polluted city.32 Interestingly, APOE-4 carriers from the polluted areas failed to identify 24 percent on the 10 items reported to be particularly sensitive to Alzheimer’s disease,33 whereas carriers of the APOE 2/3 and 3/3 alleles, which are not risk factors for Alzheimer’s disease, failed only 13.6 percent of such items, suggesting that AOE-4 gene carriers are more susceptible to adverse influences of pollution on their olfactory pathways.
Association with Parkinson’s
In the 1990s, G. Webster Ross and his collaborators at the University of Hawaii administered the 12-item version of the UPSIT to 2,276 non-symptomatic elderly men (average age: 80) of Japanese ancestry.34 Over the next four years, 35 were clinically diagnosed with Parkinson’s disease, a disorder whose motor dysfunction is due to damage to areas of the brain that employ the neurotransmitter dopamine for motor control. After adjusting for age, smoking behavior, and other confounders, those persons whose initial olfactory test scores fell within the bottom 25 percent of the group were five times more likely to develop Parkinson’s disease than those whose test scores fell within the top 25 percent.
Additional support for early olfactory involvement in Parkinson’s disease came from a 2004 study performed at the Vrije Universiteit (VU University) in Amsterdam. In this study, olfactory tests were administered to 361 asymptomatic first-degree relatives of Parkinson’s disease patients.35 The health of regions of the brain involved in motor control also was determined using single photon emission tomography (SPECT) imaging. This procedure measures the concentration of dopamine transporter, the protein responsible for returning the neurotransmitter into cells after its release into the synaptic cleft (see Figure 4). Those with the best (top 10 percent) and worse (bottom 10 percent) olfactory test scores were followed over time to determine who developed Parkinson’s disease.
Figure 5: Imaging of the dopamine receptor in patients with Parkinson’s disease (PD) (Right) and age-and sex matched normal controls (Left). Note the depletion of the radioactively labelled ligand sensitive to the dopamine transporter in the PD subjects relative to the controls. Photograph courtesy of Jacob Dubroff, Smell and Taste Center and Department of Neuroradiology, University of Pennsylvania.
Two years into the study, four of the 40 relatives (10 percent) with the worst olfactory test scores developed clinical Parkinson’s disease, whereas none of the 38 relatives with the best test scores did. By five years, the incidence among relatives rose to 12.5 percent. Only those from the poor-smelling group evidenced decreased imaging of the dopamine transporter and, in some cases, such decreases were evident at baseline, suggesting that subclinical disease had already begun. These data suggested that the risk of developing Parkinson’s disease in the presence of hyposmia may be as high as 22 percent in first-degree relatives.35
Numerous other studies support the view that olfactory testing may be helpful in predicting the development of cognitive and motor disorders.24 Indeed, olfactory dysfunction rivals and even exceeds the sensitivity of a number of other biomarkers in such prediction, including SPECT imaging of the dopamine transporter,36 as described above. Currently, novel methods are being developed to enhance the predictive power of olfactory tests. For example, spraying the inside of the nose with atropine, a drug that accentuates cognitive dysfunction in patients with Alzheimer’s disease via its anticholinergic effects, may induce a greater degree of smell loss in individuals who are at risk for future dementia, in effect “unmasking” the disease.37
Although quantitative smell testing is rarely performed by most physicians, it has been found to be useful in not only detecting, but also discriminating among, a number of neurodegenerative diseases. For example, a disorder called progressive supranuclear palsy (PSP) is often misdiagnosed as Parkinson’s disease. Unlike Parkinson’s, however, patients with PSP have a relatively normal sense of smell.38 Thus, a neurologist whose evaluation of such a person is inconclusive can use smell testing to aid in making the correct diagnosis. The same is true for distinguishing between depression and Alzheimer’s disease, with depressed patients showing little evidence of smell loss.39 In a position paper, the quality standards committee of the American Academy of Neurology has in fact recommended that olfactory testing be considered to differentiate Parkinson’s disease from PSP and corticobasal degeneration, another neurological disorder.40
Keeping Your Sense of Smell Sharp
How can each of us maintain a healthy sense of smell? All through life, viruses, air pollutants, and other environmental toxins cumulatively damage receptor cells In the uppermost regions of our noses. Such cumulative damage is not manifested until later in life, when few cells are left to provide a normal sense of smell. Hence, the degree to which we can minimize exposure to such agents, such as having good air filters in our homes and washing our hands regularly, can go a long way in preventing damage.
Maintaining good sleep patterns also protects smell function. Obstructive sleep apnea, in particular, has been associated with smell loss,41 which may be attenuated by the use of a CPAP (continuous positive airway pressure) machine at night.42 Importantly, daily exercise has been shown to help avert age-related decrements in the ability to smell.43 It may even help preserve olfaction in persons with Parkinson’s disease.44
Aside from maintaining good health via exercise, sleep, and avoidance of pathogens, a healthy diet and certain dietary interventions may also help. Gopinath and associates at the University of Sydney compared the odor identification ability of 1331 persons who differed in terms of their dietary intake of nuts, fish, butter, and margarine.45 Those with the most nut and fish consumption had a reduced likelihood of olfactory loss, possibly because of the anti-inflammatory properties of these foods‘ constituents. Similarly, Richard Stevenson and his colleagues at Macquarie University in Sydney found that persons who ate a Western style diet high in saturated fat and sugar exhibited poorer odor identification test scores than those whose diets were low in these nutrients.46
Conversely, an impaired sense of smell may lead to dietary changes that ultimately impact health, as evidenced by a study at Yale University that assessed dietary habits in 80 elderly women, 37 of whom had olfactory dysfunction.47 The latter exhibited a nutrient intake profile that increases the chances for cardiac disease, including a higher intake of sweets and a lower preference for citrus fruits.
A Tie to Coffee
My own colleagues and I showed, in 2007, that the lifetime history of coffee drinking was positively associated with UPSIT scores in relatives of patients with Parkinson’s disease.48 Thus, after correcting for age, gender, and tobacco use, the mean UPSIT score for those who drank less than one cup a day was 30.4 (out of a possible 40); for those who drank one cup a day it was 32.6, while for those who drank two to three cups a day or four or more cups a day the mean scores were 33.1 and 34.1, respectively. This pattern was statistically significant (p < 0.009) and was stronger in men than in women. Whether the same relationship may be found in the general population has yet to be determined.
Looking Forward
What does the future hold? In Japan, a major pharmaceutical company has begun an initiative to educate physicians about the importance of this primary sensory system and to distribute olfactory tests via pharmacies to promote better understanding of the health of the Japanese elderly population. In light of recent discoveries, it is inevitable that more and more physicians will begin to pay attention to the smell ability of their patients, and to routinely test this faculty.
Given that olfactory receptors are not just confined to the nose, future research will establish whether smell testing can provide information on the distribution of olfactory receptors elsewhere in the body and indicate whether such information may aid in the detection and treatment of some genetic-related diseases. More research on how odors influence mood and behavior is underway, and novel devices for adding odors to the environment are in development.
Just as we largely control our auditory environment, we may soon be able to engineer our olfactory environment in a much more sophisticated way, to alter our states of mind and improve our mental health. The future of olfactory research seems on target to fulfill the prescient assessment of Alexander Graham Bell in a 1927 Scientific Monthly article: “Odors are becoming more and more important in the world of scientific experiments and in medicine—and the need for more knowledge of odors will bring more knowledge, as surely as the sun shines.”
1. Buck L and Axel R (1991) A novel multigene family may encode odorant receptors: a molecular basis for odor recognition. Cell 65 (1):175-187
2. Greer PL, Bear DM, Lassance JM, Bloom ML, Tsukahara T, Pashkovski SL, Masuda FK, Nowlan AC, Kirchner R, Hoekstra HE, and Datta SR (2016) A Family of non-GPCR chemosensors defines an alternative logic for mammalian olfaction. Cell 165 (7):1734-1748
3. Busse D, Kudella P, Gruning NM, Gisselmann G, Stander S, Luger T, Jacobsen F, Steinstrasser L, Paus R, Gkogkolou P, Bohm M, Hatt H, and Benecke H (2014) A synthetic sandalwood odorant induces wound-healing processes in human keratinocytes via the olfactory receptor OR2AT4. J Invest Dermatol 134 (11):2823-2832
4. Pavlath GK (2010) A new function for odorant receptors: MOR23 is necessary for normal tissue repair in skeletal muscle. Cell Adh Migr 4 (4):502-506
5. Kang N, Kim H, Jae Y, Lee N, Ku CR, Margolis F, Lee EJ, Bahk YY, Kim MS, and Koo J (2015) Olfactory marker protein expression is an indicator of olfactory receptor-associated events in non-olfactory tissues. PLoS One 10 (1):e0116097
6. Foster SR, Roura E, Molenaar P, and Thomas WG (2015) G protein-coupled receptors in cardiac biology: old and new receptors. Biophys Rev 7 (1):77-89
7. Trotier D, Bensimon JL, Herman P, Tran Ba HP, Doving KB, and Eloit C (2007) Inflammatory obstruction of the olfactory clefts and olfactory loss in humans: a new syndrome? Chem Senses 32 (3):285-292
8. Kang N, Bahk YY, Lee N, Jae Y, Cho YH, Ku CR, Byun Y, Lee EJ, Kim MS, and Koo J (2015) Olfactory receptor Olfr544 responding to azelaic acid regulates glucagon secretion in alpha-cells of mouse pancreatic islets. Biochem Biophys Res Commun 460 (3):616-621
9. Kudyakova TI, Sarycheva NY, and Kamenskii AA (2007) Orientation and exploratory behavior and anxiety of CBA mice with anosmia induced by N-trimethylindole (skatole). Bull Exp Biol Med 143 (1):1-4
10. Massberg D, Jovancevic N, Offermann A, Simon A, Baniahmad A, Perner S, Pungsrinont T, Luko K, Philippou S, Ubrig B, Heiland M, Weber L, Altmuller J, Becker C, Gisselmann G, Gelis L, and Hatt H (2016) The activation of OR51E1 causes growth suppression of human prostate cancer cells. Oncotarget 7 (30):48231-48249
11. Shepard BD, Cheval L, Peterlin Z, Firestein S, Koepsell H, Doucet A, and Pluznick JL (2016) A Renal Olfactory Receptor Aids in Kidney Glucose Handling. Sci Rep 6:35215
12. Braun T, Voland P, Kunz L, Prinz C, and Gratzl M (2007) Enterochromaffin cells of the human gut: sensors for spices and odorants. Gastroenterology 132 (5):1890-1901
13. Weber M, Pehl U, Breer H, and Strotmann J (2002) Olfactory receptor expressed in ganglia of the autonomic nervous system. J Neurosci Res 68 (2):176-184
14. Chen Z, Zhao H, Fu N, and Chen L (2017) The diversified function and potential therapy of ectopic olfactory receptors in non-olfactory tissues. J Cell Physiol
15. Air Force Instructions 48-123. Accession, Retention and Administration. Medical Examination and Standards, Volume 2, 5 June 2006.
16. Doty, R. L. Handbook of Olfaction and Gustation. 3rd, 1-1217. 2015. Hoboken, N.J., John Wiley & Sons, Inc.
17. Doty RL, Shaman P, Applebaum SL, Giberson R, Siksorski L, and Rosenberg L (1984) Smell identification ability: changes with age. Science 226:1441-1443
18. Doty RL, Shaman P, and Dann M (1984) Development of the University of Pennsylvania Smell Identification Test: a standardized microencapsulated test of olfactory function. Physiology & Behavior 32:489-502
20. Stevens JC and Cain WS (1986) Aging Impairs the Ability to Perceive Gas Odor. Chemical Senses 11 (4):668
21. Pence TS, Reiter ER, DiNardo LJ, and Costanzo RM (2014) Risk factors for hazardous events in olfactory-impaired patients. JAMA Otolaryngol Head Neck Surg 140 (10):951-955
22. Devanand DP, Lee S, Manly J, Andrews H, Schupf N, Masurkar A, Stern Y, Mayeux R, and Doty RL (2015) Olfactory identification deficits and increased mortality in the community. Ann Neurol 78 (3):401-411
23. Pinto JM, Wroblewski KE, Kern DW, Schumm LP, and McClintock MK (2014) Olfactory dysfunction predicts 5-year mortality in older adults. PLoS One 9 (10):e107541
24. Doty RL, Hawkes CH, Good KP, and Duda JE (2015) Odor perception and neuropathology in neurodegenerative diseases and schizophrenia. In: Doty RL (ed) Handbook of Olfaction and Gustation. John Wiley & Sons, Hoboken, pp 403-452
25. Braak H, Braak E, Yilmazer D, de Vos RAI, Jansen ENH, and Bohl J (1996) Pattern of brain destruction in Parkinson's and Alzheimer's diseases. J Neural Trans 103:455-490
26. Doty RL (2017) Olfactory dysfunction in neurodegenerative diseases: is there a common pathological substrate? Lancet neurol 16 (6):478-488
27. Sohrabi HR, Bates KA, Rodrigues M, Taddei K, Laws SM, Lautenschlager NT, Dhaliwal SS, Johnston AN, Mackay-Sim A, Gandy S, Foster JK, and Martins RN (2009) Olfactory dysfunction is associated with subjective memory complaints in community-dwelling elderly individuals. J Alzheimers Dis 17 (1):135-142
28. Devanand DP, Tabert MH, Cuasay K, Manly JJ, Schupf N, Brickman AM, Andrews H, Brown TR, DeCarli C, and Mayeux R (2010) Olfactory identification deficits and MCI in a multi-ethnic elderly community sample. Neurobiol Aging 31 (9):1593-1600
29. Devanand DP, Lee S, Manly J, Andrews H, Schupf N, Doty RL, Stern Y, Zahodne LB, Louis ED, and Mayeux R (2015) Olfactory deficits predict cognitive decline and Alzheimer dementia in an urban community. Neurology 84 (2):182-189
30. Graves AB, Bowen JD, Rajaram L, McCormick WC, McCurry SM, Schellenberg GD, and Larson EB (1999) Impaired olfaction as a marker for cognitive decline: interaction with apolipoprotein E epsilon4 status. Neurology 53 (7):1480-1487
31. Serby M, Mohan C, Aryan M, Williams L, Mohs RC, and Davis KL (1996) Olfactory identification deficits in relatives of Alzheimer's disease patients. Biol Psychiat 39 (5):375-377
32. Calderon-Garciduenas L, Franco-Lira M, Henriquez-Roldan C, Osnaya N, Gonzalez-Maciel A, Reynoso-Robles R, Villarreal-Calderon R, Herritt L, Brooks D, Keefe S, Palacios-Moreno J, Villarreal-Calderon R, Torres-Jardon R, Medina-Cortina H, Delgado-Chavez R, Aiello-Mora M, Maronpot RR, and Doty RL (2010) Urban air pollution: Influences on olfactory function and pathology in exposed children and young adults. Experimental and Toxicological Pathology 62:91-102
33. Tabert MH, Liu X, Doty RL, Serby M, Zamora D, Pelton GH, Marder K, Albers MW, Stern Y, and Devanand DP (2005) A 10-item smell identification scale related to risk for Alzheimer's disease. Ann Neurol 58 (1):155-160
34. Ross GW, Petrovitch H, Abbott RD, Tanner CM, Popper J, Masaki K, Launer L, and White LR (2008) Association of olfactory dysfunction with risk for future Parkinson's disease. Ann Neurol 63 (2):167-173
35. Ponsen MM, Stoffers D, Wolters EC, Booij J, and Berendse HW (2010) Olfactory testing combined with dopamine transporter imaging as a method to detect prodromal Parkinson's disease. J Neurol Neurosurg Psychiatry 81 (4):396-399
36. Deeb J, Shah M, Muhammed N, Gunasekera R, Gannon K, Findley LJ, and Hawkes CH (2010) A basic smell test is as sensitive as a dopamine transporter scan: comparison of olfaction, taste and DaTSCAN in the diagnosis of Parkinson's disease. Quarterly Journal of Medicine 103 (12):941-952
37. Schofield PW, Ebrahimi H, Jones AL, Bateman GA, and Murray SR (2012) An olfactory 'stress test' may detect preclinical Alzheimer's disease. BMC Neurol 12:24
38. Doty RL, Golbe LI, McKeown DA, Stern MB, Lehrach CM, and Crawford D (1993) Olfactory testing differentiates between progressive supranuclear palsy and idiopathic Parkinson's disease. Neurology 43 (5):962-965
39. Solomon GS, Petrie WM, Hart JR, and Brackin HB, Jr. (1998) Olfactory dysfunction discriminates Alzheimer's dementia from major depression. Journal of Neuropsychiatry & Clinical Neurosciences 1998 Winter;10 (1):64-67
40. Suchowersky O, Reich S, Perlmutter J, Zesiewicz T, Gronseth G, and Weiner WJ (2006) Practice Parameter: Diagnosis and prognosis of new onset Parkinson disease (an evidence-based review) Report of the Quality Standards Subcommittee of the American Academy of Neurology. Neurology 66 (7):968-975
41. Salihoglu M, Kendirli MT, Altundag A, Tekeli H, Saglam M, Cayonu M, Senol MG, and Ozdag F (2014) The effect of obstructive sleep apnea on olfactory functions. Laryngoscope 124 (9):2190-2194
42. Walliczek-Dworschak U, Cassel W, Mittendorf L, Pellegrino R, Koehler U, Guldner C, Dworschak POG, Hildebrandt O, Daniel H, Gunzel T, Teymoortash A, and Hummel T (2017) Continuous positive air pressure improves orthonasal olfactory function of patients with obstructive sleep apnea. Sleep Med 34:24-29
43. Schubert CR, Fischer ME, Pinto AA, Klein BEK, Klein R, and Cruickshanks KJ (2017) Odor detection thresholds in a population of older adults. Laryngoscope 127 (6):1257-1262
44. Rosenfeldt AB, Dey T, and Alberts JL (2016) Aerobic Exercise Preserves Olfaction Function in Individuals with Parkinson's Disease. Parkinsons Dis 2016:9725089
45. Gopinath B, Sue CM, Flood VM, Burlutsky G, and Mitchell P (2015) Dietary intakes of fats, fish and nuts and olfactory impairment in older adults. Br J Nutr 114 (2):240-247
46. Stevenson RJ, Boakes RA, Oaten MJ, Yeomans MR, Mahmut M, and Francis HM (2016) Chemosensory Abilities in Consumers of a Western-Style Diet. Chem Senses 41 (6):505-513
47. Duffy VB, Backstrand JR, and Ferris AM (1995) Olfactory dysfunction and related nutritional risk in free-living, elderly women. J Am Diet Assoc 95 (8):879-884
48. Siderowf A, Jennings D, Connolly J, Doty RL, Marek K, and Stern MB (2007) Risk factors for Parkinson's disease and impaired olfaction in relatives of patients with Parkinson's disease. Mov Disord 22 (15):2249-2255
49. Menco BPM and Morrison EE (2003) Morphology of the mammalian olfactory epithelium: form, fine structure, function, and pathology. In: Doty RL (ed) Handbook of olfaction and gustation. Marcel Dekker, New York, pp 17-49
50. Fusar-Poli P, Rubia K, Rossi G, Sartori G, and Balottin U (2012) Striatal dopamine transporter alterations in ADHD: pathophysiology or adaptation to psychostimulants? A meta-analysis. Am J Psychiatry 169 (3):264-272
More comfortable online than out partying, post-Millennials are safer, physically, than adolescents have ever been. But they’re on the brink of a mental-health crisis.
One day last summer, around noon, I called Athena, a 13-year-old who lives in Houston, Texas. She answered her phone—she’s had an iPhone since she was 11—sounding as if she’d just woken up. We chatted about her favorite songs and TV shows, and I asked her what she likes to do with her friends. “We go to the mall,” she said. “Do your parents drop you off?,” I asked, recalling my own middle-school days, in the 1980s, when I’d enjoy a few parent-free hours shopping with my friends. “No—I go with my family,” she replied. “We’ll go with my mom and brothers and walk a little behind them. I just have to tell my mom where we’re going. I have to check in every hour or every 30 minutes.”
Those mall trips are infrequent—about once a month. More often, Athena and her friends spend time together on their phones, unchaperoned. Unlike the teens of my generation, who might have spent an evening tying up the family landline with gossip, they talk on Snapchat, the smartphone app that allows users to send pictures and videos that quickly disappear. They make sure to keep up their Snapstreaks, which show how many days in a row they have Snapchatted with each other. Sometimes they save screenshots of particularly ridiculous pictures of friends. “It’s good blackmail,” Athena said. (Because she’s a minor, I’m not using her real name.) She told me she’d spent most of the summer hanging out alone in her room with her phone. That’s just the way her generation is, she said. “We didn’t have a choice to know any life without iPads or iPhones. I think we like our phones more than we like actual people.”
I’ve been researching generational differences for 25 years, starting when I was a 22-year-old doctoral student in psychology. Typically, the characteristics that come to define a generation appear gradually, and along a continuum. Beliefs and behaviors that were already rising simply continue to do so. Millennials, for instance, are a highly individualistic generation, but individualism had been increasing since the Baby Boomers turned on, tuned in, and dropped out. I had grown accustomed to line graphs of trends that looked like modest hills and valleys. Then I began studying Athena’s generation.
Around 2012, I noticed abrupt shifts in teen behaviors and emotional states. The gentle slopes of the line graphs became steep mountains and sheer cliffs, and many of the distinctive characteristics of the Millennial generation began to disappear. In all my analyses of generational data—some reaching back to the 1930s—I had never seen anything like it.
At first I presumed these might be blips, but the trends persisted, across several years and a series of national surveys. The changes weren’t just in degree, but in kind. The biggest difference between the Millennials and their predecessors was in how they viewed the world; teens today differ from the Millennials not just in their views but in how they spend their time. The experiences they have every day are radically different from those of the generation that came of age just a few years before them.
What happened in 2012 to cause such dramatic shifts in behavior? It was after the Great Recession, which officially lasted from 2007 to 2009 and had a starker effect on Millennials trying to find a place in a sputtering economy. But it was exactly the moment when the proportion of Americans who owned a smartphone surpassed 50 percent.
The more I pored over yearly surveys of teen attitudes and behaviors, and the more I talked with young people like Athena, the clearer it became that theirs is a generation shaped by the smartphone and by the concomitant rise of social media. I call them iGen. Born between 1995 and 2012, members of this generation are growing up with smartphones, have an Instagram account before they start high school, and do not remember a time before the internet. The Millennials grew up with the web as well, but it wasn’t ever-present in their lives, at hand at all times, day and night. iGen’s oldest members were early adolescents when the iPhone was introduced, in 2007, and high-school students when the iPad entered the scene, in 2010. A 2017 survey of more than 5,000 American teens found that three out of four owned an iPhone.
The advent of the smartphone and its cousin the tablet was followed quickly by hand-wringing about the deleterious effects of “screen time.” But the impact of these devices has not been fully appreciated, and goes far beyond the usual concerns about curtailed attention spans. The arrival of the smartphone has radically changed every aspect of teenagers’ lives, from the nature of their social interactions to their mental health. These changes have affected young people in every corner of the nation and in every type of household. The trends appear among teens poor and rich; of every ethnic background; in cities, suburbs, and small towns. Where there are cell towers, there are teens living their lives on their smartphone.
To those of us who fondly recall a more analog adolescence, this may seem foreign and troubling. The aim of generational study, however, is not to succumb to nostalgia for the way things used to be; it’s to understand how they are now. Some generational changes are positive, some are negative, and many are both. More comfortable in their bedrooms than in a car or at a party, today’s teens are physically safer than teens have ever been. They’re markedly less likely to get into a car accident and, having less of a taste for alcohol than their predecessors, are less susceptible to drinking’s attendant ills.
Psychologically, however, they are more vulnerable than Millennials were: Rates of teen depression and suicide have skyrocketed since 2011. It’s not an exaggeration to describe iGen as being on the brink of the worst mental-health crisis in decades. Much of this deterioration can be traced to their phones.
Even when a seismic event—a war, a technological leap, a free concert in the mud—plays an outsize role in shaping a group of young people, no single factor ever defines a generation. Parenting styles continue to change, as do school curricula and culture, and these things matter. But the twin rise of the smartphone and social media has caused an earthquake of a magnitude we’ve not seen in a very long time, if ever. There is compelling evidence that the devices we’ve placed in young people’s hands are having profound effects on their lives—and making them seriously unhappy.
In the early 1970s, the photographer Bill Yates shot a series of portraits at the Sweetheart Roller Skating Rink in Tampa, Florida. In one, a shirtless teen stands with a large bottle of peppermint schnapps stuck in the waistband of his jeans. In another, a boy who looks no older than 12 poses with a cigarette in his mouth. The rink was a place where kids could get away from their parents and inhabit a world of their own, a world where they could drink, smoke, and make out in the backs of their cars. In stark black-and-white, the adolescent Boomers gaze at Yates’s camera with the self-confidence born of making your own choices—even if, perhaps especially if, your parents wouldn’t think they were the right ones.
Fifteen years later, during my own teenage years as a member of Generation X, smoking had lost some of its romance, but independence was definitely still in. My friends and I plotted to get our driver’s license as soon as we could, making DMV appointments for the day we turned 16 and using our newfound freedom to escape the confines of our suburban neighborhood. Asked by our parents, “When will you be home?,” we replied, “When do I have to be?”
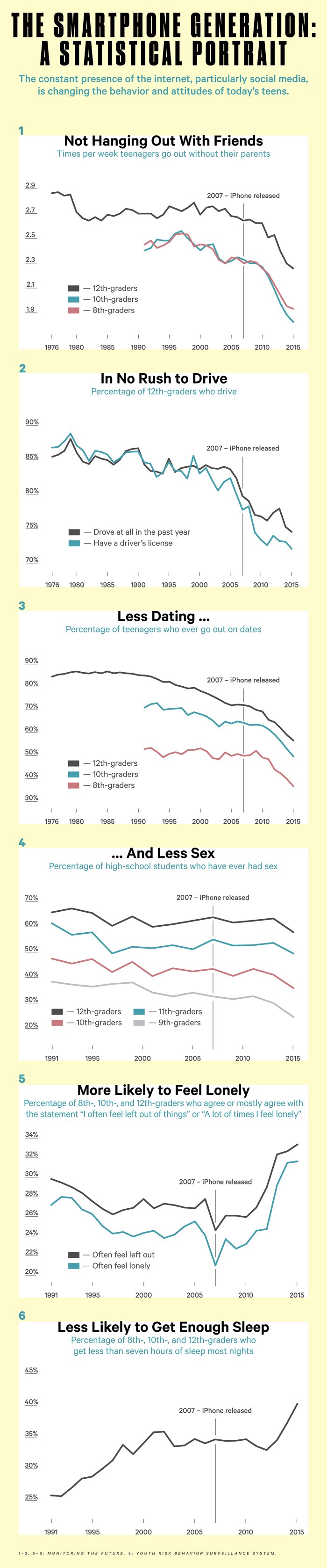
But the allure of independence, so powerful to previous generations, holds less sway over today’s teens, who are less likely to leave the house without their parents. The shift is stunning: 12th-graders in 2015 were going out less often than eighth-graders did as recently as 2009.
Today’s teens are also less likely to date. The initial stage of courtship, which Gen Xers called “liking” (as in “Ooh, he likes you!”), kids now call “talking”—an ironic choice for a generation that prefers texting to actual conversation. After two teens have “talked” for a while, they might start dating. But only about 56 percent of high-school seniors in 2015 went out on dates; for Boomers and Gen Xers, the number was about 85 percent.
The decline in dating tracks with a decline in sexual activity. The drop is the sharpest for ninth-graders, among whom the number of sexually active teens has been cut by almost 40 percent since 1991. The average teen now has had sex for the first time by the spring of 11th grade, a full year later than the average Gen Xer. Fewer teens having sex has contributed to what many see as one of the most positive youth trends in recent years: The teen birth rate hit an all-time low in 2016, down 67 percent since its modern peak, in 1991.
Even driving, a symbol of adolescent freedom inscribed in American popular culture, from Rebel Without a Cause to Ferris Bueller’s Day Off, has lost its appeal for today’s teens. Nearly all Boomer high-school students had their driver’s license by the spring of their senior year; more than one in four teens today still lack one at the end of high school. For some, Mom and Dad are such good chauffeurs that there’s no urgent need to drive. “My parents drove me everywhere and never complained, so I always had rides,” a 21-year-old student in San Diego told me. “I didn’t get my license until my mom told me I had to because she could not keep driving me to school.” She finally got her license six months after her 18th birthday. In conversation after conversation, teens described getting their license as something to be nagged into by their parents—a notion that would have been unthinkable to previous generations.
Independence isn’t free—you need some money in your pocket to pay for gas, or for that bottle of schnapps. In earlier eras, kids worked in great numbers, eager to finance their freedom or prodded by their parents to learn the value of a dollar. But iGen teens aren’t working (or managing their own money) as much. In the late 1970s, 77 percent of high-school seniors worked for pay during the school year; by the mid-2010s, only 55 percent did. The number of eighth-graders who work for pay has been cut in half. These declines accelerated during the Great Recession, but teen employment has not bounced back, even though job availability has.
Of course, putting off the responsibilities of adulthood is not an iGen innovation. Gen Xers, in the 1990s, were the first to postpone the traditional markers of adulthood. Young Gen Xers were just about as likely to drive, drink alcohol, and date as young Boomers had been, and more likely to have sex and get pregnant as teens. But as they left their teenage years behind, Gen Xers married and started careers later than their Boomer predecessors had.
Gen X managed to stretch adolescence beyond all previous limits: Its members started becoming adults earlier and finished becoming adults later. Beginning with Millennials and continuing with iGen, adolescence is contracting again—but only because its onset is being delayed. Across a range of behaviors—drinking, dating, spending time unsupervised— 18-year-olds now act more like 15-year-olds used to, and 15-year-olds more like 13-year-olds. Childhood now stretches well into high school.
Why are today’s teens waiting longer to take on both the responsibilities and the pleasures of adulthood? Shifts in the economy, and parenting, certainly play a role. In an information economy that rewards higher education more than early work history, parents may be inclined to encourage their kids to stay home and study rather than to get a part-time job. Teens, in turn, seem to be content with this homebody arrangement—not because they’re so studious, but because their social life is lived on their phone. They don’t need to leave home to spend time with their friends.
If today’s teens were a generation of grinds, we’d see that in the data. But eighth-, 10th-, and 12th-graders in the 2010s actually spend less time on homework than Gen X teens did in the early 1990s. (High-school seniors headed for four-year colleges spend about the same amount of time on homework as their predecessors did.) The time that seniors spend on activities such as student clubs and sports and exercise has changed little in recent years. Combined with the decline in working for pay, this means iGen teens have more leisure time than Gen X teens did, not less.
So what are they doing with all that time? They are on their phone, in their room, alone and often distressed.
Jasu Hu
One of the ironies of iGen life is that despite spending far more time under the same roof as their parents, today’s teens can hardly be said to be closer to their mothers and fathers than their predecessors were. “I’ve seen my friends with their families—they don’t talk to them,” Athena told me. “They just say ‘Okay, okay, whatever’ while they’re on their phones. They don’t pay attention to their family.” Like her peers, Athena is an expert at tuning out her parents so she can focus on her phone. She spent much of her summer keeping up with friends, but nearly all of it was over text or Snapchat. “I’ve been on my phone more than I’ve been with actual people,” she said. “My bed has, like, an imprint of my body.”
In this, too, she is typical. The number of teens who get together with their friends nearly every day dropped by more than 40 percent from 2000 to 2015; the decline has been especially steep recently. It’s not only a matter of fewer kids partying; fewer kids are spending time simply hanging out. That’s something most teens used to do: nerds and jocks, poor kids and rich kids, C students and A students. The roller rink, the basketball court, the town pool, the local necking spot—they’ve all been replaced by virtual spaces accessed through apps and the web.
You might expect that teens spend so much time in these new spaces because it makes them happy, but most data suggest that it does not. The Monitoring the Future survey, funded by the National Institute on Drug Abuse and designed to be nationally representative, has asked 12th-graders more than 1,000 questions every year since 1975 and queried eighth- and 10th-graders since 1991. The survey asks teens how happy they are and also how much of their leisure time they spend on various activities, including nonscreen activities such as in-person social interaction and exercise, and, in recent years, screen activities such as using social media, texting, and browsing the web. The results could not be clearer: Teens who spend more time than average on screen activities are more likely to be unhappy, and those who spend more time than average on nonscreen activities are more likely to be happy.
There’s not a single exception. All screen activities are linked to less happiness, and all nonscreen activities are linked to more happiness. Eighth-graders who spend 10 or more hours a week on social media are 56 percent more likely to say they’re unhappy than those who devote less time to social media. Admittedly, 10 hours a week is a lot. But those who spend six to nine hours a week on social media are still 47 percent more likely to say they are unhappy than those who use social media even less. The opposite is true of in-person interactions. Those who spend an above-average amount of time with their friends in person are 20 percent less likely to say they’re unhappy than those who hang out for a below-average amount of time.
If you were going to give advice for a happy adolescence based on this survey, it would be straightforward: Put down the phone, turn off the laptop, and do something—anything—that does not involve a screen. Of course, these analyses don’t unequivocally prove that screen time causes unhappiness; it’s possible that unhappy teens spend more time online. But recent research suggests that screen time, in particular social-media use, does indeed cause unhappiness. One study asked college students with a Facebook page to complete short surveys on their phone over the course of two weeks. They’d get a text message with a link five times a day, and report on their mood and how much they’d used Facebook. The more they’d used Facebook, the unhappier they felt, but feeling unhappy did not subsequently lead to more Facebook use.
Social-networking sites like Facebook promise to connect us to friends. But the portrait of iGen teens emerging from the data is one of a lonely, dislocated generation. Teens who visit social-networking sites every day but see their friends in person less frequently are the most likely to agree with the statements “A lot of times I feel lonely,” “I often feel left out of things,” and “I often wish I had more good friends.” Teens’ feelings of loneliness spiked in 2013 and have remained high since.
This doesn’t always mean that, on an individual level, kids who spend more time online are lonelier than kids who spend less time online. Teens who spend more time on social media also spend more time with their friends in person, on average—highly social teens are more social in both venues, and less social teens are less so. But at the generational level, when teens spend more time on smartphones and less time on in-person social interactions, loneliness is more common.
So is depression. Once again, the effect of screen activities is unmistakable: The more time teens spend looking at screens, the more likely they are to report symptoms of depression. Eighth-graders who are heavy users of social media increase their risk of depression by 27 percent, while those who play sports, go to religious services, or even do homework more than the average teen cut their risk significantly.
Teens who spend three hours a day or more on electronic devices are 35 percent more likely to have a risk factor for suicide, such as making a suicide plan. (That’s much more than the risk related to, say, watching TV.) One piece of data that indirectly but stunningly captures kids’ growing isolation, for good and for bad: Since 2007, the homicide rate among teens has declined, but the suicide rate has increased. As teens have started spending less time together, they have become less likely to kill one another, and more likely to kill themselves. In 2011, for the first time in 24 years, the teen suicide rate was higher than the teen homicide rate.
Depression and suicide have many causes; too much technology is clearly not the only one. And the teen suicide rate was even higher in the 1990s, long before smartphones existed. Then again, about four times as many Americans now take antidepressants, which are often effective in treating severe depression, the type most strongly linked to suicide.
What’s the connection between smartphones and the apparent psychological distress this generation is experiencing? For all their power to link kids day and night, social media also exacerbate the age-old teen concern about being left out. Today’s teens may go to fewer parties and spend less time together in person, but when they do congregate, they document their hangouts relentlessly—on Snapchat, Instagram, Facebook. Those not invited to come along are keenly aware of it. Accordingly, the number of teens who feel left out has reached all-time highs across age groups. Like the increase in loneliness, the upswing in feeling left out has been swift and significant.
This trend has been especially steep among girls. Forty-eight percent more girls said they often felt left out in 2015 than in 2010, compared with 27 percent more boys. Girls use social media more often, giving them additional opportunities to feel excluded and lonely when they see their friends or classmates getting together without them. Social media levy a psychic tax on the teen doing the posting as well, as she anxiously awaits the affirmation of comments and likes. When Athena posts pictures to Instagram, she told me, “I’m nervous about what people think and are going to say. It sometimes bugs me when I don’t get a certain amount of likes on a picture.”
Girls have also borne the brunt of the rise in depressive symptoms among today’s teens. Boys’ depressive symptoms increased by 21 percent from 2012 to 2015, while girls’ increased by 50 percent—more than twice as much. The rise in suicide, too, is more pronounced among girls. Although the rate increased for both sexes, three times as many 12-to-14-year-old girls killed themselves in 2015 as in 2007, compared with twice as many boys. The suicide rate is still higher for boys, in part because they use more-lethal methods, but girls are beginning to close the gap.
These more dire consequences for teenage girls could also be rooted in the fact that they’re more likely to experience cyberbullying. Boys tend to bully one another physically, while girls are more likely to do so by undermining a victim’s social status or relationships. Social media give middle- and high-school girls a platform on which to carry out the style of aggression they favor, ostracizing and excluding other girls around the clock.
Social-media companies are of course aware of these problems, and to one degree or another have endeavored to prevent cyberbullying. But their various motivations are, to say the least, complex. A recently leaked Facebook document indicated that the company had been touting to advertisers its ability to determine teens’ emotional state based on their on-site behavior, and even to pinpoint “moments when young people need a confidence boost.” Facebook acknowledged that the document was real, but denied that it offers “tools to target people based on their emotional state.”
In July 2014, a 13-year-old girl in North Texas woke to the smell of something burning. Her phone had overheated and melted into the sheets. National news outlets picked up the story, stoking readers’ fears that their cellphone might spontaneously combust. To me, however, the flaming cellphone wasn’t the only surprising aspect of the story. Why, I wondered, would anyone sleep with her phone beside her in bed? It’s not as though you can surf the web while you’re sleeping. And who could slumber deeply inches from a buzzing phone?
Curious, I asked my undergraduate students at San Diego State University what they do with their phone while they sleep. Their answers were a profile in obsession. Nearly all slept with their phone, putting it under their pillow, on the mattress, or at the very least within arm’s reach of the bed. They checked social media right before they went to sleep, and reached for their phone as soon as they woke up in the morning (they had to—all of them used it as their alarm clock). Their phone was the last thing they saw before they went to sleep and the first thing they saw when they woke up. If they woke in the middle of the night, they often ended up looking at their phone. Some used the language of addiction. “I know I shouldn’t, but I just can’t help it,” one said about looking at her phone while in bed. Others saw their phone as an extension of their body—or even like a lover: “Having my phone closer to me while I’m sleeping is a comfort.”
It may be a comfort, but the smartphone is cutting into teens’ sleep: Many now sleep less than seven hours most nights. Sleep experts say that teens should get about nine hours of sleep a night; a teen who is getting less than seven hours a night is significantly sleep deprived. Fifty-seven percent more teens were sleep deprived in 2015 than in 1991. In just the four years from 2012 to 2015, 22 percent more teens failed to get seven hours of sleep.
The increase is suspiciously timed, once again starting around when most teens got a smartphone. Two national surveys show that teens who spend three or more hours a day on electronic devices are 28 percent more likely to get less than seven hours of sleep than those who spend fewer than three hours, and teens who visit social-media sites every day are 19 percent more likely to be sleep deprived. A meta-analysis of studies on electronic-device use among children found similar results: Children who use a media device right before bed are more likely to sleep less than they should, more likely to sleep poorly, and more than twice as likely to be sleepy during the day.
Electronic devices and social media seem to have an especially strong ability to disrupt sleep. Teens who read books and magazines more often than the average are actually slightly less likely to be sleep deprived—either reading lulls them to sleep, or they can put the book down at bedtime. Watching TV for several hours a day is only weakly linked to sleeping less. But the allure of the smartphone is often too much to resist.
Sleep deprivation is linked to myriad issues, including compromised thinking and reasoning, susceptibility to illness, weight gain, and high blood pressure. It also affects mood: People who don’t sleep enough are prone to depression and anxiety. Again, it’s difficult to trace the precise paths of causation. Smartphones could be causing lack of sleep, which leads to depression, or the phones could be causing depression, which leads to lack of sleep. Or some other factor could be causing both depression and sleep deprivation to rise. But the smartphone, its blue light glowing in the dark, is likely playing a nefarious role.
The correlations between depression and smartphone use are strong enough to suggest that more parents should be telling their kids to put down their phone. As the technology writer Nick Bilton has reported, it’s a policy some Silicon Valley executives follow. Even Steve Jobs limited his kids’ use of the devices he brought into the world.
What’s at stake isn’t just how kids experience adolescence. The constant presence of smartphones is likely to affect them well into adulthood. Among people who suffer an episode of depression, at least half become depressed again later in life. Adolescence is a key time for developing social skills; as teens spend less time with their friends face-to-face, they have fewer opportunities to practice them. In the next decade, we may see more adults who know just the right emoji for a situation, but not the right facial expression.
I realize that restricting technology might be an unrealistic demand to impose on a generation of kids so accustomed to being wired at all times. My three daughters were born in 2006, 2009, and 2012. They’re not yet old enough to display the traits of iGen teens, but I have already witnessed firsthand just how ingrained new media are in their young lives. I’ve observed my toddler, barely old enough to walk, confidently swiping her way through an iPad. I’ve experienced my 6-year-old asking for her own cellphone. I’ve overheard my 9-year-old discussing the latest app to sweep the fourth grade. Prying the phone out of our kids’ hands will be difficult, even more so than the quixotic efforts of my parents’ generation to get their kids to turn off MTV and get some fresh air. But more seems to be at stake in urging teens to use their phone responsibly, and there are benefits to be gained even if all we instill in our children is the importance of moderation. Significant effects on both mental health and sleep time appear after two or more hours a day on electronic devices. The average teen spends about two and a half hours a day on electronic devices. Some mild boundary-setting could keep kids from falling into harmful habits.
In my conversations with teens, I saw hopeful signs that kids themselves are beginning to link some of their troubles to their ever-present phone. Athena told me that when she does spend time with her friends in person, they are often looking at their device instead of at her. “I’m trying to talk to them about something, and they don’t actually look at my face,” she said. “They’re looking at their phone, or they’re looking at their Apple Watch.” “What does that feel like, when you’re trying to talk to somebody face-to-face and they’re not looking at you?,” I asked. “It kind of hurts,” she said. “It hurts. I know my parents’ generation didn’t do that. I could be talking about something super important to me, and they wouldn’t even be listening.”
Once, she told me, she was hanging out with a friend who was texting her boyfriend. “I was trying to talk to her about my family, and what was going on, and she was like, ‘Uh-huh, yeah, whatever.’ So I took her phone out of her hands and I threw it at my wall.”
I couldn’t help laughing. “You play volleyball,” I said. “Do you have a pretty good arm?” “Yep,” she replied.
What I Needed From the Church During My Depression
3 ways our communities can support mental health.
Alicia Cohn | posted August 3, 2016
Image: Milos Kreckovic / iStock
Speaking at the Democratic National Convention last week, the singer Demi Lovato took advantage of the powerful platform to advocate for mental health care in America. “Like millions of Americans, I am living with mental illness,” she said. "Too many Americans from all walks of life don't get help, either because they fear the stigma or they cannot afford treatment."
“Mental illness” is a scary-sounding category that encompasses a broad array of invisible struggles. Look around you on Sunday. Most likely, there are Christians next to you suffering silently from anxiety or panic disorder, bipolar disorder (from which Lovato suffers), dysthymia or major depressive disorder (from which I have suffered). Whether through personal experience or through someone we know, those of us whose lives have been touched by mental health struggles know that getting help can be the hardest part.
Women are twice as likely to experience mental health struggles as men, thanks to major hormonal challenges such as pregnancy and menstruation. According to the Centers for Disease Control and Prevention (CDC), 30 percent of women between 18 and 44 years of age are affected by depression, and many of them don’t get the help they need. (My own disorder went undiagnosed for almost six months before I got help from doctors and therapy, and even then, the recovery process has been hindered by bad advice, mistreatment, and poor choices about whom I can rely on.)
Unfortunately, many of us who have spoken up in church communities have been told to “pray harder” or “have more faith.” These suggestions might be well intentioned, but they often discourage and isolate those of us in desperate need of support. “It’s a knee-jerk reaction to judge people when they’re vulnerable,” wrote actress Kristen Bell of her own story. “But there’s nothing weak about struggling with mental illness. You’re just having a harder time living in your brain than other people.”
She’s right: Struggling with an illness of any kind makes a person vulnerable, and a sick brain puts a person in a particularly vulnerable state because it’s often impossible to discern the problem from the inside. The sick brain can’t see the sick brain. More often than not, someone in the midst of a depressive episode or panic attack can barely put forth a cry for help.
As people living in Christian community, we should be ready to offer practical knowledge and gracious support to people experiencing mental health crises. With that in mind, here are three ways I believe every church is best positioned to help:
Faith in something better.
“Have faith that on the other side of your pain is something good,” Dwayne “The Rock” Johnson told the Oprah Presents Master Class. He wished someone had relayed this idea to him during a low point in his life when he was “crying constantly.” His message mirrors the “It gets better” campaign, but many people suffering from depression or other mental health issues know that sometimes it gets worse. Everyone needs a reason to keep trying. I’ve been in enough therapy groups and doctors’ offices to know that the only reason people keep looking for answers in the face of crippling despair is because they believe something will help: drugs, doctors, relationships, therapy, or sometimes the sheer freedom of living at rock bottom. Nonetheless, I've seen the best results when I (and others) put faith not exclusively in doctors or drugs or therapies, which have their limits, but also in God. He is the reason I still believe in “something good” on the other side of my pain.
If you know someone in your church like me who is suffering, come alongside her. Pray for her. Avoid cheap platitudes like “have faith” and instead offer practical support by checking in on a regular basis to let her know she’s not alone, or by asking about her treatment, which is a way of acknowledging that the illness is real.
Resilience.
Millennials are on more antidepressants than any other generation. According to the CDC, more than 6 percent of 18-to 39-year-olds have been prescribed antidepressants. My generation might as well define ourselves as “behind” in our careers (40 percent of unemployed people are milennials), salaries, and personal lives (marrying late and moving back in with our parents). No wonder we’re depressed. On top of that, the hours we spend in psychiatrists’ or counselors’ offices dealing with symptoms of a disorder (or the side effects of medication) often feel like “lost” time. While dealing with my mental health problems, I have burned through a lot of time and money as well as emotional and relationship capital—all resources that I feel could have been spent better elsewhere. I find it reassuring to know that Christianity offers a promise of restoration greater than anything lost (Joel 2:25; Job 42:10–17). In the Bible, people often fall down, their lives fall apart, and yet God raises them up again.
With that in mind, if you encounter someone in your church who is struggling with suicidal ideation or any form of hopelessness, first affirm their pain, then offer them the grace of optimism.
The "seasonal" perspective.
“For now” is the mantra my therapist gave me to get through depressive episodes and hard days. Ecclesiastes 3 provides a similar mantra: “To everything there is a season.” Mental health, too, is composed of seasons. I am currently in a season for antidepressants, and although it may be cyclical, I hope it will eventually end. For most people, circumstances change, the brain’s reactions change accordingly, and the appropriate therapy also changes in sync with the situation. With mental health challenges, maintaining a long-range perspective is key to survival. The hardest, most important thing to do is simply to persevere.
If someone near you is facing a discrete mental health episode or a lifelong challenge, encourage her to name the season she’s in, remind her that seasons often change, and journey with her as she takes it one day at a time.
“I don't think I'm fixed,” Lovato shared in the MTV documentary about her “recovery” in a residential treatment facility. “People think that you're like a car in a body shop. You go in, they fix you, and you're out. It takes constant fixing."
Much like spiritual health, mental health is an ongoing need for every human being. Although those of us who struggle are each responsible for ourselves, we also rely on the powerful support of our community to ensure that we get the care we need. It starts with awareness within each local church. Just as an increasing number of secular figures have spoken up publicly, Christians should step forward to be, as Lovato put it, “proof that you can live a normal and empowered life with mental illness.”
The Bible is filled with exhortations to care for the most vulnerable among us—those who cry out for mercy and feel they have nowhere to turn. Those of us who face mental health crises are among the most vulnerable. We need your recognition. We need your prayers. We need your presence. And we need to be part of the church community, especially as we struggle to find extra grace.